
Fitness
Using Molecular Testing to Guide Perioperative Systemic Therapy for Urothelial Cancer

(UroToday.com) The 2024 American Society of Clinical Oncology (ASCO) annual meeting featured a session on optimizing treatment for your patient with urothelial cancer, and a presentation by Dr. Matt Galsky discussing the use of molecular testing to guide perioperative systemic therapy for urothelial cancer. Dr. Galsky notes that perioperative systemic therapy is among the greatest achievements in solid tumor medical oncology, but in the future, our current approach may well be viewed with skepticism. Perioperative systemic therapy is really the epitome of imprecision medicine, as we are unable to ascertain who needs treatment and who benefits from treatment. This is illustrated by the following figure highlighting who does not need adjuvant therapy, a window of patients that need adjuvant treatment, and those that need adjuvant therapy but do not benefit:
Biomarkers are ideal, but Dr. Galsky notes that we have a “Double Biomarker Dilemma” in that we have the barrier of deciding who needs treatment and who benefits from treatment (based on molecular subtypes? DDR alterations? PD-L1 IHC?). As such, we may need separate biomarkers to answer both of these questions.
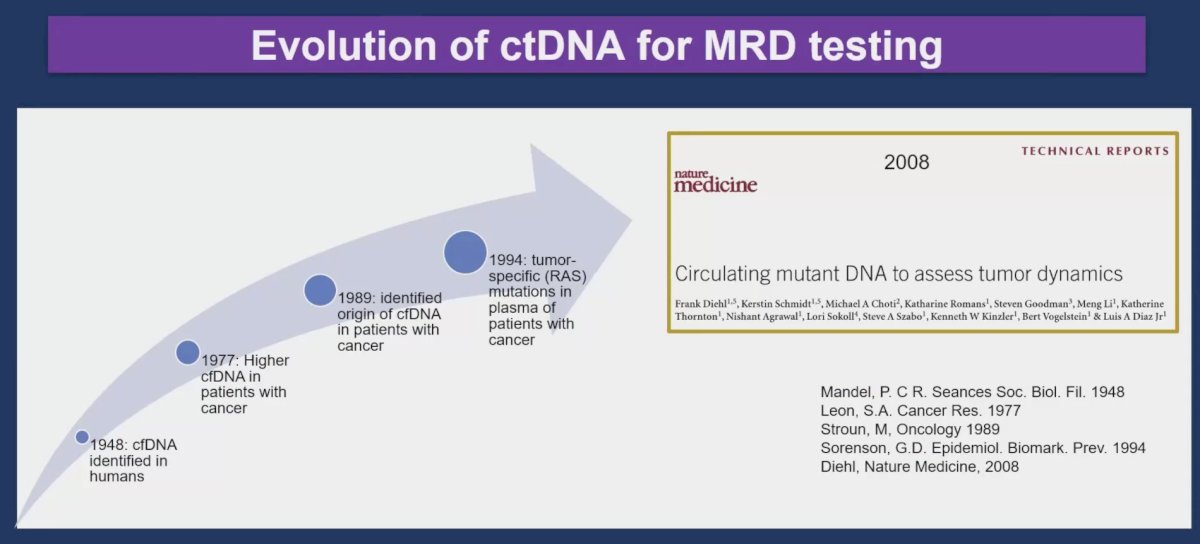
The remainder of Dr. Galsky’s talk focused on “who needs treatment”? The closest we have to a biomarker for assessing who needs perioperative treatment is molecular residual disease, with the following evolution of ctDNA for this purpose:
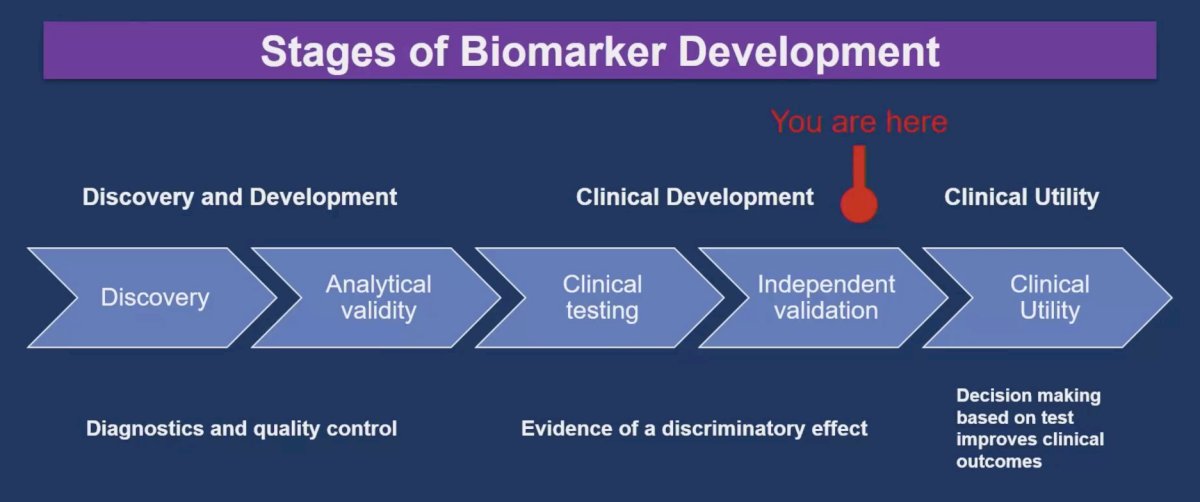
The reason this process has been decades in development is because of working through the stages of biomarker development: from discovery and development to clinical development to clinical utility:
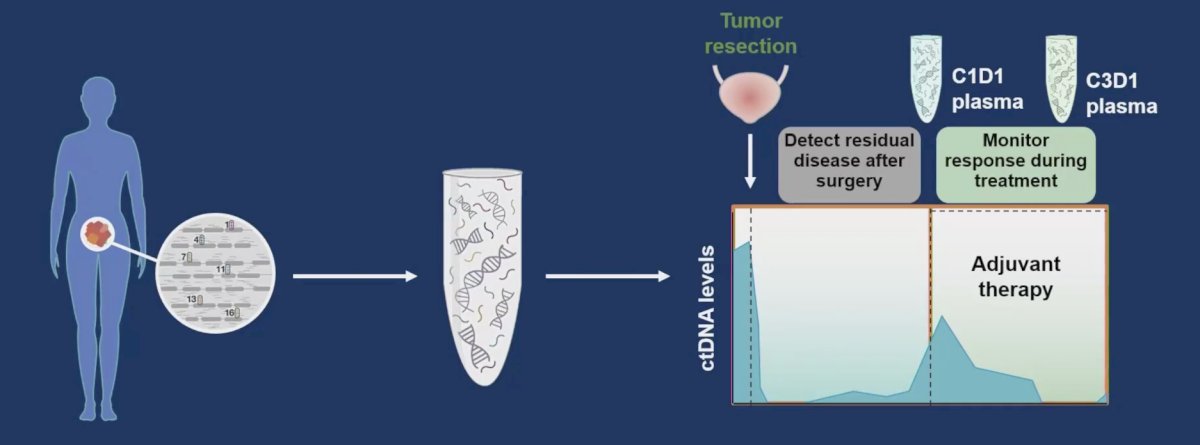
Tumor informed ctDNA testing for molecular residual disease involves DNA sequencing of the primary tumor with the following schematic:
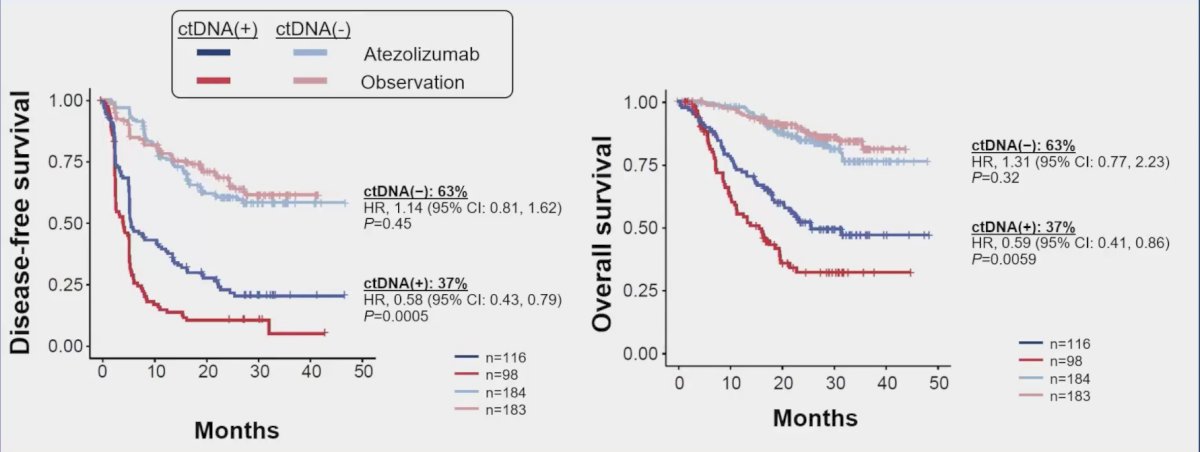
Work from Tom Powles and the IMvigor010 trial showed us that ctDNA is prognostic and predictive after adjuvant atezolizumab.1 Among 581 patients, ctDNA testing at the start of therapy (cycle 1 day 1) identified 214 (37%) patients who were positive for ctDNA and who had poor prognosis (observation arm HR 6.3, 95% CI 4.45-8.92). Notably, patients who were positive for ctDNA had improved disease-free survival and overall survival in the atezolizumab arm versus the observation arm (disease-free survival HR 0.58, 95% CI 0.43-0.79, overall survival HR 0.59, 95% CI 0.41-0.86):
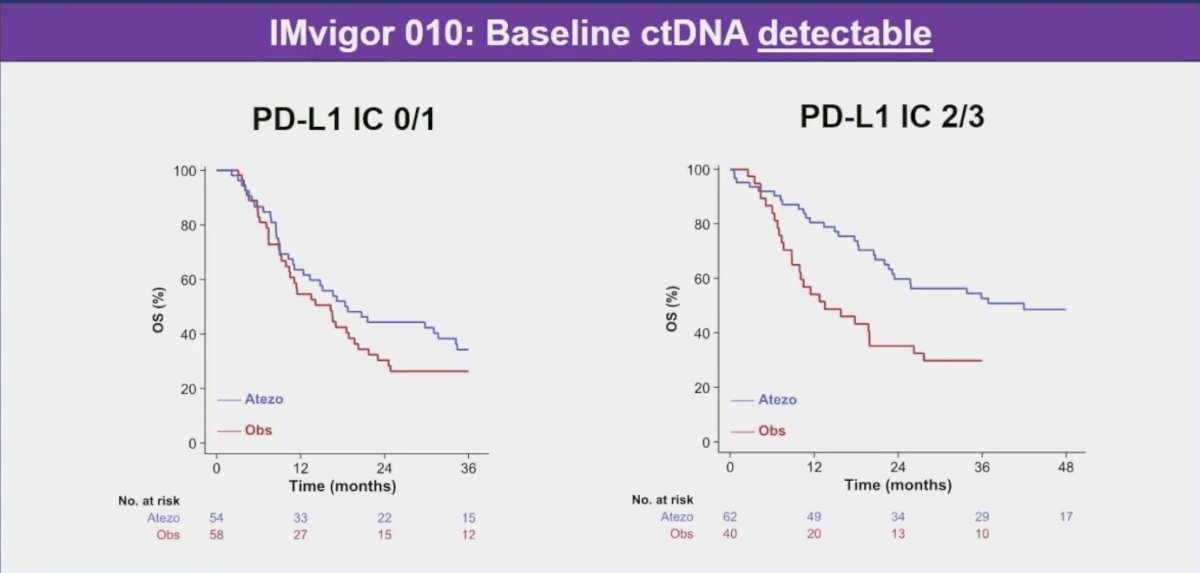
Is it possible to combine biomarkers of “need” for treatment and biomarkers of “benefit” from treatment? Dr. Galsky notes that in the IMvigor010 trial, among those patients with detectable baseline ctDNA, those with elevated PD-L1 expression (IC 2/3) appear to derive a benefit from atezolizumab compared to observation, whereas those without PD-L1 expression (IC 0/1) did not:
IMvigor 011 is an important study for the field, whereby it assesses the clinical utility of ctDNA testing in the adjuvant setting of bladder cancer. Patients with positive ctDNA are randomized 2:1 to 1 year of atezolizumab versus placebo and patients with negative ctDNA undergo observation with radiographic imaging every 6 months for 2 years. If the negative ctDNA patients convert to detectable ctDNA, they can then move to the randomization of atezolizumab versus placebo arm. The primary endpoint is investigator-assessed disease free survival and the trial design is as follows:

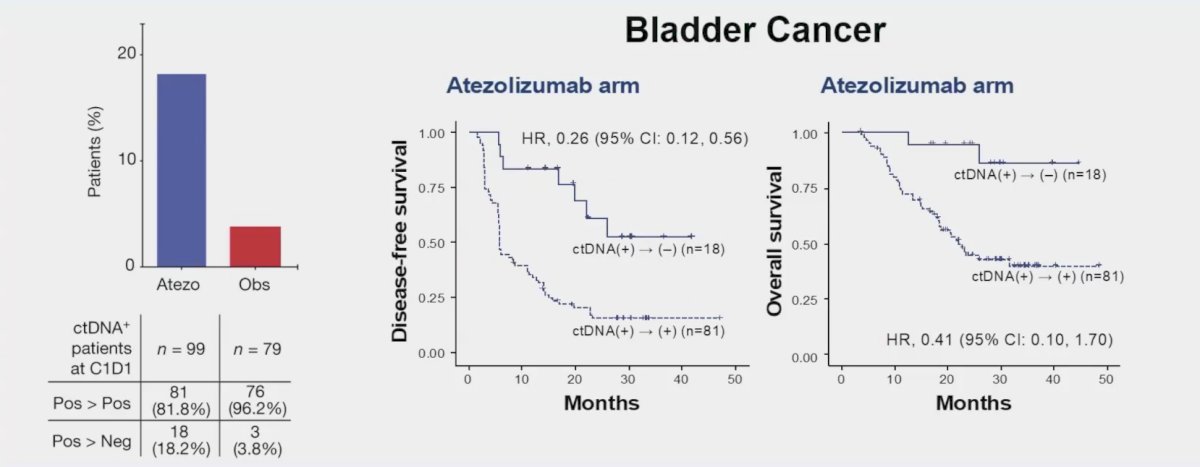
Dr. Galsky notes that serial ctDNA testing over time may also allow us to assess response to adjuvant immune checkpoint blockade, and even potentially deem a patient cured if there ctDNA remains undetectable over serial time points. ctDNA-based molecular residual disease may also serve as an intermediate clinical endpoint. Looking again at Dr. Powles work in IMvigor010, Dr. Galsky notes that assessing ctDNA patients at cycle 1/day 1 and their subsequent clearance of ctDNA may inform treatment decisions:
Recently, the FDA has provided guidance for the utilization of ctDNA, noting that ctDNA as a measure of response could be used in early phase clinical trials to aid in signal finding. Additionally, with regards to ctDNA as an early endpoint in clinical trials, the FDA states that changes in ctDNA in response to a drug may have the potential to be used as an early endpoint to support drug approval in the early stage cancer setting.
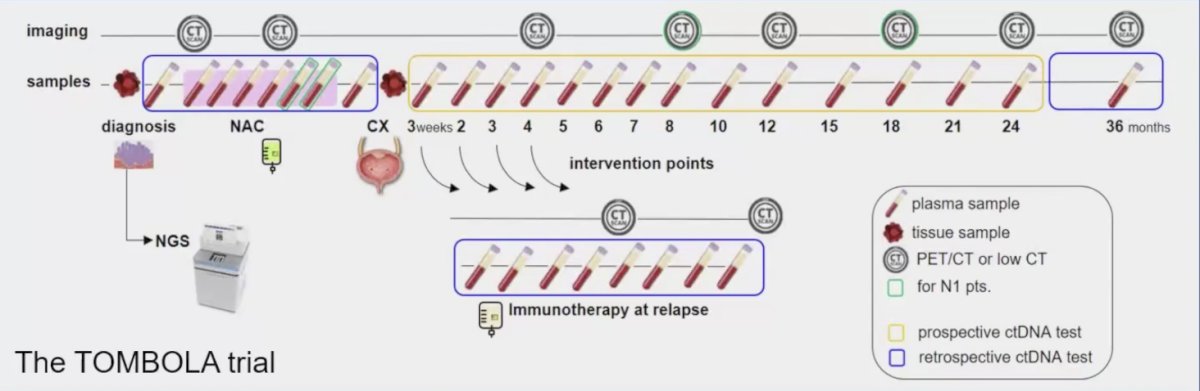
Whether a molecular recurrence is a new clinical disease state is being assessed in the TOMBOLA trial whereby patients with muscle invasive bladder cancer who are treated with neoadjuvant chemotherapy followed by cystectomy and have negative serial ctDNA following surgery are then treated with atezolizumab if there ctDNA becomes detectable. The primary endpoint for this trial is complete response as defined by negative ctDNA after atezolizumab in combination with normal imaging findings:
Dr. Galsky is the PI of the MODERN (Alliance 032103) trial of patients after cystectomy having a ctDNA assay and then those that are ctDNA positive being randomized to 12 cycles of adjuvant nivolumab versus adjuvant nivolumab + 12 cycles of relatlimab, and those patients with negative ctDNA being randomized to 12 cycles of adjuvant nivolumab versus surveillance:

There are several unanswered questions in this disease space, as highlighted by Dr. Galsky:
- What are the implications of ctDNA positivity in the pre-surgical setting?
- Is molecular residual disease a qualitative versus quantitative biomarker?
- When is the right time to test post surgery?
- What is the impact of transient versus sustained ctDNA clearance?
- Is molecular recurrence a new clinical disease state and can studies be feasibly conducted?
Dr. Galsky concluded his presentation by discussing the use of molecular testing to guide perioperative systemic therapy for urothelial cancer with the following take home messages:
- ctDNA is poised to change treatment paradigms in urothelial cancer
- Prospective studies of ctDNA guided perioperative systemic therapy are needed to establish clinical utility
Presented by: Matt D. Galsky, MD, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, May 31 – Tues, June 4, 2024.
References:
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021 Jl;595(7867):432-437.

From Stadium to Screen: How Technology is Changing Sports Viewing

20/7/2024 Horse Racing Tips and Best Bets – Flemington, Flemington Cup day

Indian tech hub Karnataka state’s move to reserve jobs for locals not finalised, chief minister says

Financial picture dramatically improves for Shamrock Rovers in 48 hours with Sinclair Armstrong deal and European win

Our fashion editor’s favourite affordable bag is 20% off today

Jay Shah’s Big Decision Hovers Over Cricket’s Associate Member Directors Election

Budget shampoo that adds MAJOR volume boost is on sale for Amazon Prime Day: ‘Your hair feels fuller and thicker’

Being active on your commute lowers risk of disease and mental health

Tiger Woods cops brutal Open schedule as full Round 1 tee times revealed
