
Tech
Post Hoc Analysis of ARASENS

(UroToday.com) The 2024 American Society of Clinical Oncology (ASCO) annual meeting featured a session on prostate cancer, and a presentation by Dr. Marc-Oliver Grimm discussing a post hoc analysis of ARASENS discussing post-progression survival of patients with metastatic hormone-sensitive prostate cancer (mHSPC) who received darolutamide or placebo. Darolutamide is a structurally distinct and highly potent androgen receptor pathway inhibitor with low blood brain barrier penetration and limited potential for drug-drug interactions. In ARASENS, the addition of darolutamide to ADT and docetaxel significantly reduced the risk of death by 32.5% in patients with mHSPC,1 despite most placebo patients (75.6%) receiving subsequent therapy. Darolutamide also delayed time to progression to metastatic castration-resistant prostate cancer (mCRPC; median, not reached vs 19.1 months for placebo), resulting in a longer time in mHSPC, which is associated with improved quality of life versus mCRPC. At ASCO 2024, Dr. Grimm and colleagues reported post-progression subsequent anticancer therapies and related survival from ARASENS.
Patients with mHSPC were randomized 1:1 to darolutamide 600 mg twice daily or placebo in addition to ADT + docetaxel. After treatment discontinuation, patients entered active and long-term survival follow-up periods during which assessments included subsequent therapies and survival outcomes. Post-progression survival was defined as time from first subsequent therapy to death using Kaplan-Meier estimates.
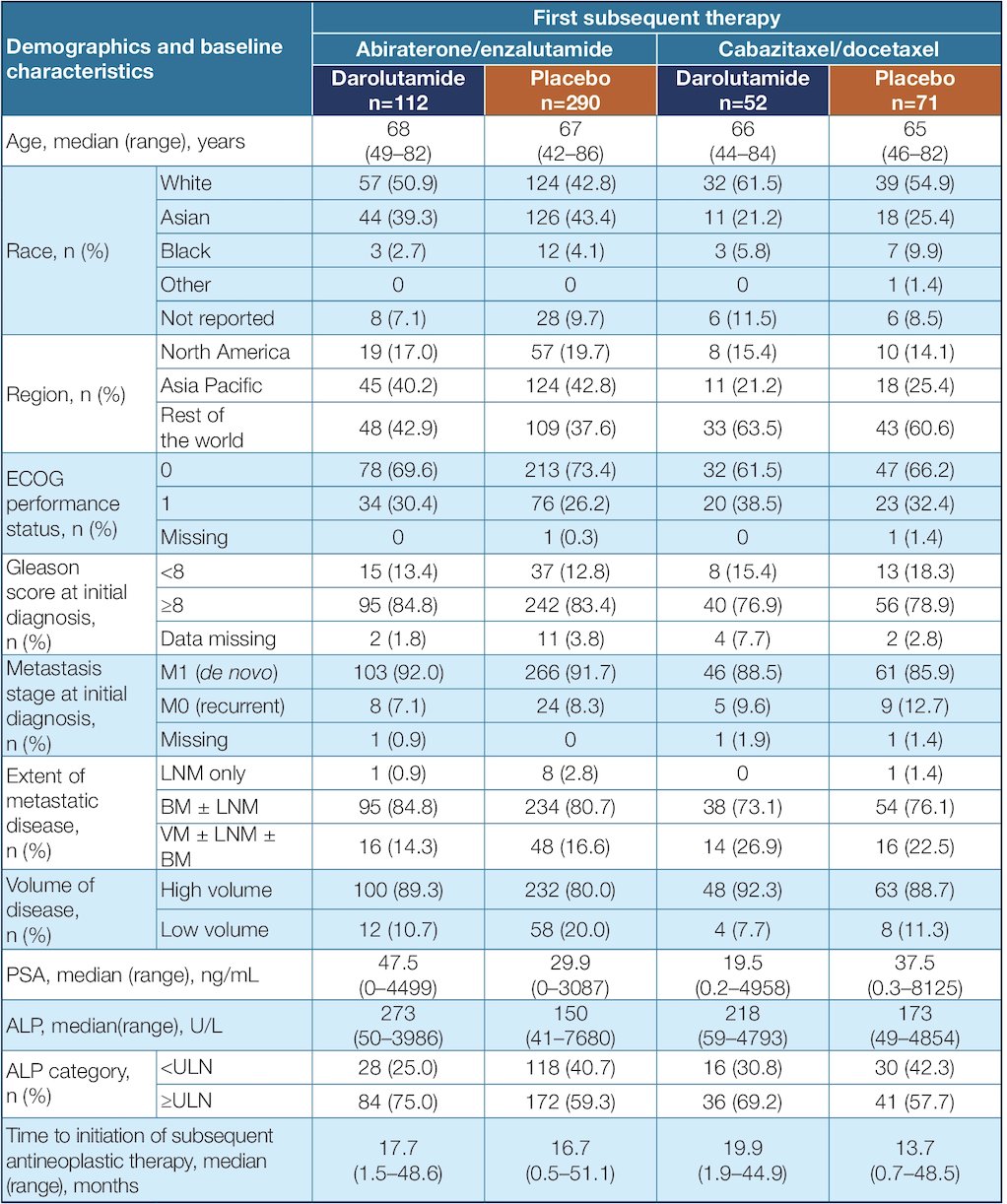
Among 1,305 treated patients (darolutamide n = 651; placebo n = 654), 315 receiving darolutamide and 495 receiving placebo entered follow-up. Among these patients, 57% (n = 179) and 76% (n = 374), respectively, received subsequent therapy. This included abiraterone and enzalutamide as the most frequent first subsequent therapy:
The five most common post-progression first subsequent anticancer therapies (in descending order) were abiraterone, enzalutamide, cabazitaxel, docetaxel, and radium-223. In the darolutamide arm, 90% of first subsequent therapies were androgen receptor pathway inhibitor or chemotherapy. In contrast, in the placebo arm, the majority (78%) received first subsequent therapy with either enzalutamide or abiraterone. Patient demographics and baseline characteristics were generally similar between the darolutamide and placebo groups within the first subsequent therapy subpopulations:
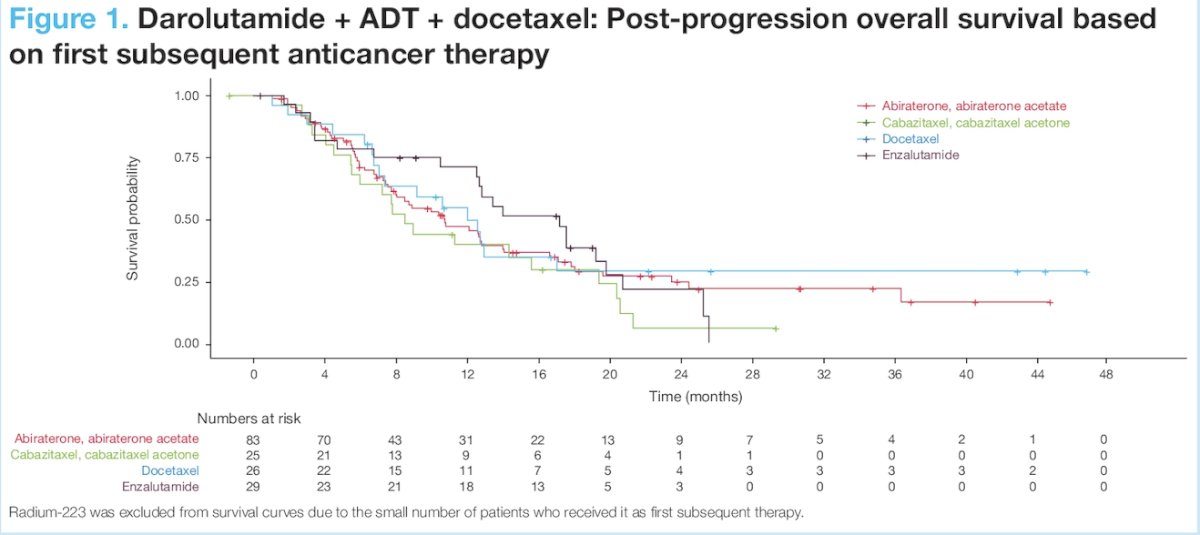
For patients receiving darolutamide + ADT + docetaxel, minimal difference was observed in post-progression survival between subsequent therapies, suggesting subsequent therapy with another androgen receptor pathway inhibitor does not provide further survival benefit vs non-androgen receptor pathway inhibitor options (mainly chemotherapy):
For patients who received placebo + ADT + docetaxel, post-progression survival was improved when the majority (78%) received a first subsequent anticancer therapy with a different mechanism of action. The median post-progression survival was 23.0 months with androgen receptor pathway inhibitor therapy and 13.5 months with non-androgen receptor pathway inhibitor subsequent therapy:

Patients receiving darolutamide + ADT + docetaxel stayed on treatment for more than 2 years longer than those receiving placebo + ADT + docetaxel, and median overall survival time was not reached in the darolutamide group:

Dr. Grimm concluded his presentation by discussing a post hoc analysis of ARASENS discussing post-progression survival of patients with mHSPC who received darolutamide or placebo with the following take home messages:
- Darolutamide + ADT + docetaxel increased overall survival versus placebo + ADT + docetaxel and also delayed time to progression to mCRPC
- For patients receiving darolutamide + ADT + docetaxel for mHSPC, post-progression survival was similar independent of subsequent anticancer therapy with an androgen receptor pathway inhibitor or chemotherapy
- Patients receiving placebo + ADT + docetaxel mostly sequenced to an androgen receptor pathway inhibitor, and this first androgen receptor pathway inhibitor exposure provided a post-progression survival benefit versus subsequent non- androgen receptor pathway inhibitor therapies
- The greater overall survival benefit and delay in disease progression to mCRPC were observed when treatment was intensified with the darolutamide combination
Presented by: Marc-Oliver Grimm, MD, Jena University Hospital, Jena, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting, Chicago, IL, Fri, May 31 – Tues, June 4, 2024.
References:

From Stadium to Screen: How Technology is Changing Sports Viewing

20/7/2024 Horse Racing Tips and Best Bets – Flemington, Flemington Cup day

Indian tech hub Karnataka state’s move to reserve jobs for locals not finalised, chief minister says

Financial picture dramatically improves for Shamrock Rovers in 48 hours with Sinclair Armstrong deal and European win

Our fashion editor’s favourite affordable bag is 20% off today

Jay Shah’s Big Decision Hovers Over Cricket’s Associate Member Directors Election

Budget shampoo that adds MAJOR volume boost is on sale for Amazon Prime Day: ‘Your hair feels fuller and thicker’

Being active on your commute lowers risk of disease and mental health

Tiger Woods cops brutal Open schedule as full Round 1 tee times revealed
