
Fitness
A Prospective Cohort Study of Antimony Exposure and Cognitive Impairment in Older Adults — China, 2017–2021
Antimony (Sb) has been identified as a novel neurotoxin that affects neurocognition in previous animal studies. However, there is limited research on the association between Sb exposure and cognitive impairment in humans. Given the increasing aging population, it is crucial to investigate the relationship between Sb and cognitive impairment in older adults. In this study, we utilized data from the Healthy Aging and Biomarkers Cohort Study (HABCS), a prospective cohort study. A total of 1,333 participants aged 65 years and older were recruited in 2017–2018 and followed up in 2020–2021. Blood Sb (B-Sb) and urine Sb (U-Sb) concentrations were measured using inductively coupled plasma mass spectrometry. Cognitive function was assessed using the validated Mini-Mental State Examination. During the follow-up period of 4,972.1 person-years, 241 cases of cognitive impairments were recorded. Cox regression models, adjusted for potential covariates, showed that the risk of cognitive impairment increased by 56.5% for each e-fold increase in U-Sb. Similar results were observed for B-Sb, with a 52.3% increase in the risk of cognitive impairment for each e-fold increase. Our findings suggest that reducing Sb exposure may help mitigate the burden of cognitive impairment, particularly in regions with high Sb pollution.
The participants were selected from the HABCS study (1), which was conducted in nine regions known for longevity between 2017 and 2018. Follow-up of participants took place between 2020 and 2021. Detailed information about the nine longevity regions can be found in the
The study participants were divided into two groups based on their cognitive function. Continuous variables with a normal distribution were presented as mean±standard deviation (SD), while those with a skewed distribution were described as median (P25–P75). The t-test or rank sum test was used to analyze continuous variables, while categorical variables were described as frequencies (percentages) and analyzed using the χ2-test. A correlation map was used to represent the relationship between the independent variable and the covariable. A strong correlation was defined as |r|>0.7, indicating the possibility of multicollinearity. However, no statistically significant correlations were observed between variables in the correlation map (
A total of 1,333 participants were enrolled in the study from 2020 to 2021, with an average follow-up duration of 3.73±0.21 years. Among these participants, 1,092 (81.9%) had normal cognitive function, while 241 (18.1%) had cognitive impairment. The median (P25–P75) levels of B-Sb and U-Sb exposure were 2.98 (2.45–3.72) μg/L and 0.05 (0.05–0.19) μg/L, respectively (
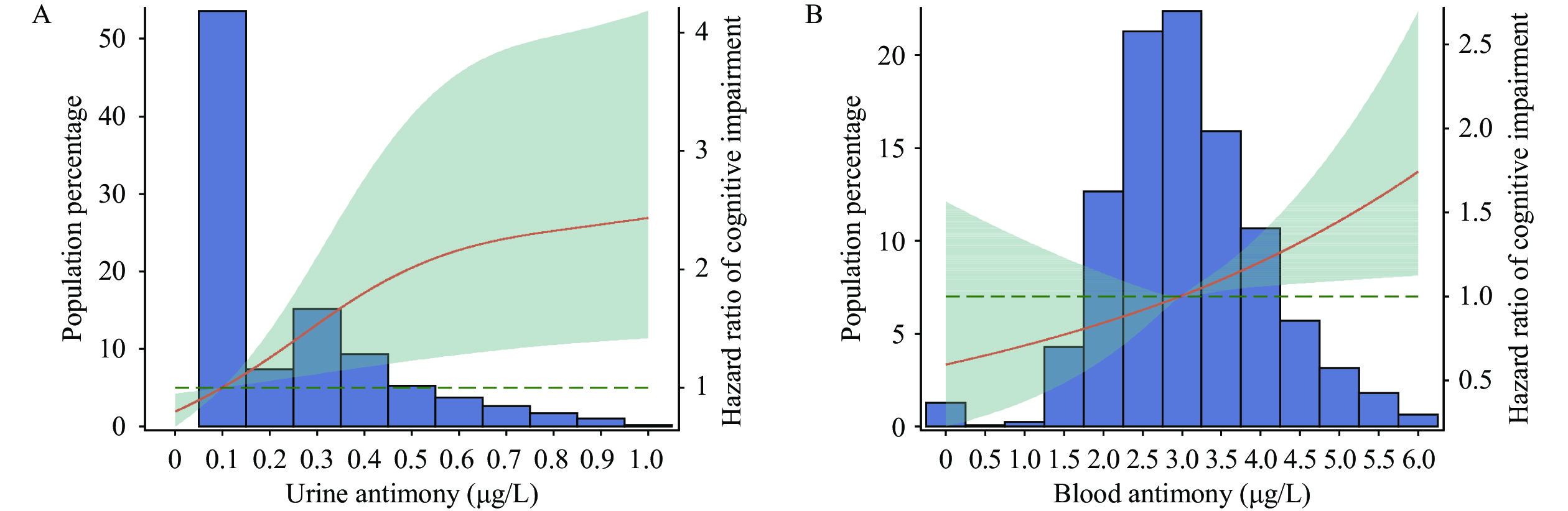
After controlling for all covariates, we observed that the risk of cognitive impairment increased by 56.5% with each e-fold increase in U-Sb [hazard ratio (HR)=1.565, 95% confidence interval (CI): 1.230, 1.991]. Compared to the low U-Sb group, the HR (95% CI) for cognitive impairment in the high U-Sb group was 2.456 (1.536, 3.927) (Table 1, Model 4). The non-linear relationship between U-Sb and the risk of cognitive impairment in older adults was confirmed by restricted cubic spline analysis (PnonlinearFigure 1A). Furthermore, the risk of cognitive impairment in older adults increased linearly with B-Sb exposure, with a 52.3% increased risk for each e-fold increase in B-Sb (HR=1.523, 95% CI: 1.100, 2.109) (Figure 1B, Table 1).
| Antimony | HR (95% CI) | ||||
| Crude model | Model 1 | Model 2 | Model 3 | Model 4 | |
| Ln-transformed B-Sb§ | 1.189 (0.906, 1.559) | 1.179 (0.866, 1.605) | 1.121 (0.830, 1.515) | 1.235 (0.865, 1.765) | 1.523 (1.100, 2.109)* |
| Categorical by concentration | |||||
| Low group | 1.000 reference | 1.000 reference | 1.000 reference | 1.000 reference | 1.000 reference |
| Medium group | 1.086 (0.789, 1.496) | 1.045 (0.752, 1.451) | 1.031 (0.735, 1.447) | 1.128 (0.788, 1.613) | 1.183 (0.822, 1.704) |
| High group | 1.229 (0.891, 1.694) | 1.239 (0.890, 1.726) | 1.140 (0.810, 1.604) | 1.213 (0.844, 1.745) | 1.300 (0.890, 1.899) |
| P for trend | 0.209 | 0.204 | 0.452 | 0.296 | 0.174 |
| Ln-transformed U-Sb¶ | 1.323 (1.127, 1.553)† | 1.312 (1.100, 1.565)† | 1.309 (1.084, 1.580)† | 1.353 (1.105, 1.658)† | 1.565 (1.230, 1.991)† |
| Categorical by concentration | |||||
| Low group | 1.000 reference | 1.000 reference | 1.000 reference | 1.000 reference | 1.000 reference |
| Medium group | 1.476 (1.060, 2.056)* | 1.392 (0.970, 1.996) | 1.363 (0.932, 1.993) | 1.495 (0.989, 2.259) | 1.403 (0.913, 2.156) |
| High group | 1.683 (1.216, 2.330)† | 1.774 (1.238, 2.542)† | 1.708 (1.173, 2.488)† | 1.874 (1.243, 2.825)† | 2.456 (1.536, 3.927)† |
| P for trend | 0.002 | 0.005 | 0.002 | ||
| Abbreviation: B-Sb=blood antimony; U-Sb=urine antimony; HR=hazard ratio; CI=confidence interval. * Denotes statistical significance at P† Denotes statistical significance at P§ low group (0.04≤B-Sb≤2.45 μg/L), medium group (2.45 |
|||||
Table 1.
Association of antimony with cognitive impairment among Chinese older adults from 2017 to 2021.
{kind=link}
Association of antimony with cognitive impairment among Chinese older adults from 2017 to 2021 in Cox models with restricted cubic spline. (A) the dose-response relationship between urine antimony levels and cognitive impairment; (B) the dose-response relationship between blood antimony levels and cognitive impairment.
Note: In Figure 1A, the plot contains three knots located at the 50th, 75th, and 95th centiles; the red line represents the estimated effect of urine antimony on the risk of cognitive impairment, while the green areas indicate the corresponding 95% confidence interval; the effect estimates were adjusted for several covariates, including urine creatinine, age, sex, ethnicity, marital status, residence, cigarette smoking, alcohol drinking, dietary intake of fruit, fish, milk, and nuts, BMI, CVD, hypertension, diabetes, CKD, urine As, urine Cd, urine Se, urine Hg, urine Pb, and urine Mn. In Figure 1B, three knots were observed at the 25th, 50th, and 75th centiles; the estimated effect of blood antimony on the risk of cognitive impairment in older adults is represented by the red line, while the green areas indicate the 95% confidence interval; Adjusted covariates include age, sex, ethnicity, marital status, place of residence, cigarette smoking, alcohol drinking, fruit, fish, milk, and nuts, BMI, CVD, hypertension, diabetes, CKD, blood As, blood Cd, blood Se, blood Hg, blood Pb, and blood Mn.
In the subgroup analysis, we observed a stronger impact of Sb exposure on cognitive impairment in individuals aged 65–79 years, men, and individuals who consume alcohol. Among smokers, the effect of U-Sb on cognitive impairment was higher compared to non-smokers. We found a significant interaction effect between B-Sb and sex, but no significant interactions were observed between age, cigarette smoking, alcohol drinking, and Sb exposure (Table 2). The results of four sensitivity analyses further supported the robustness of our findings (
| Subgroup | Ln-transformed B-Sb (HR, 95% CI)§ | Pinteraction | Ln-transformed U-Sb (HR, 95% CI) | Pinteraction |
| Age, years | 0.433 | 0.072 | ||
| 65–79 (n=759) | 2.577 (1.235, 5.377)* | 1.859 (1.106, 3.125)* | ||
| ≥80 (n=574) | 1.242 (0.829, 1.861) | 1.557 (1.174, 2.064)† | ||
| Sex | 0.048 | 0.666 | ||
| Men (n=703) | 2.458 (1.416, 4.267)† | 1.733 (1.243, 2.416)† | ||
| Women (n=630) | 1.041 (0.681, 1.592) | 1.293 (0.899, 1.860) | ||
| Cigarette smoking | 0.375 | 0.175 | ||
| Smoker (n=423) | 2.015 (0.974, 4.169) | 2.099 (1.345, 3.278)† | ||
| Non-smoker (n=904) | 1.445 (0.972, 2.147) | 1.536 (1.116, 2.116)† | ||
| Alcohol drinking | 0.123 | 0.653 | ||
| Drinker (n=390) | 2.705 (1.075, 6.807)* | 1.891 (1.145, 3.123)* | ||
| Non-drinker (n=934) | 1.346 (0.964, 1.881) | 1.431 (1.046, 1.957)* | ||
| Abbreviation: B-Sb=blood antimony; U-Sb=urine antimony; HR=hazard ratio; CI=confidence interval. * Denotes statistical significance at P† Denotes statistical significance at P§ Model was adjusted for age, sex, ethnicity, marriage status, residence, cigarette smoking, alcohol drinking, the consumption of fruit, fish, milk, and nuts, BMI, CVD, hypertension, diabetes, CKD, blood As, blood Cd, blood Se, blood Hg, blood Pb, and blood Mn. ¶ Model was adjusted for urine creatinine, age, sex, ethnicity, marriage status, residence, cigarette smoking, alcohol drinking, the consumption of fruit, fish, milk, and nuts, BMI, CVD, hypertension, diabetes, CKD, urine As, urine Cd, urine Se, urine Hg, urine Pb, and urine Mn. |
||||
Table 2.
Association of antimony with cognitive impairment among Chinese older adults in selected population subgroups from 2017 to 2021.

From Stadium to Screen: How Technology is Changing Sports Viewing

20/7/2024 Horse Racing Tips and Best Bets – Flemington, Flemington Cup day

Indian tech hub Karnataka state’s move to reserve jobs for locals not finalised, chief minister says

Financial picture dramatically improves for Shamrock Rovers in 48 hours with Sinclair Armstrong deal and European win

Our fashion editor’s favourite affordable bag is 20% off today

Jay Shah’s Big Decision Hovers Over Cricket’s Associate Member Directors Election

Budget shampoo that adds MAJOR volume boost is on sale for Amazon Prime Day: ‘Your hair feels fuller and thicker’

Being active on your commute lowers risk of disease and mental health

Tiger Woods cops brutal Open schedule as full Round 1 tee times revealed
