

In a recent review published in the journal Frontiers Endocrinology, researchers collate and elucidate recent clinical and pathophysiological knowledge on Tirzepatide. This novel anti-obesity and weight loss-promoting drug is the first twincretin, composed of GLP-1 receptor (GLP1-R) and GIP-receptor (GIP-R) agonists. It has shown significant promise as an effective intervention against type 2 diabetes (T2D) and excessive body weight, resulting in the United States Food and Drug Administration (FDA) approving its use against both conditions in May 2022 for T2D and November 2023 for obesity. This review synthesizes progress in Tirzepatide research to educate clinicians and the general public about the benefits and pathophysiological underpinnings of the drug.
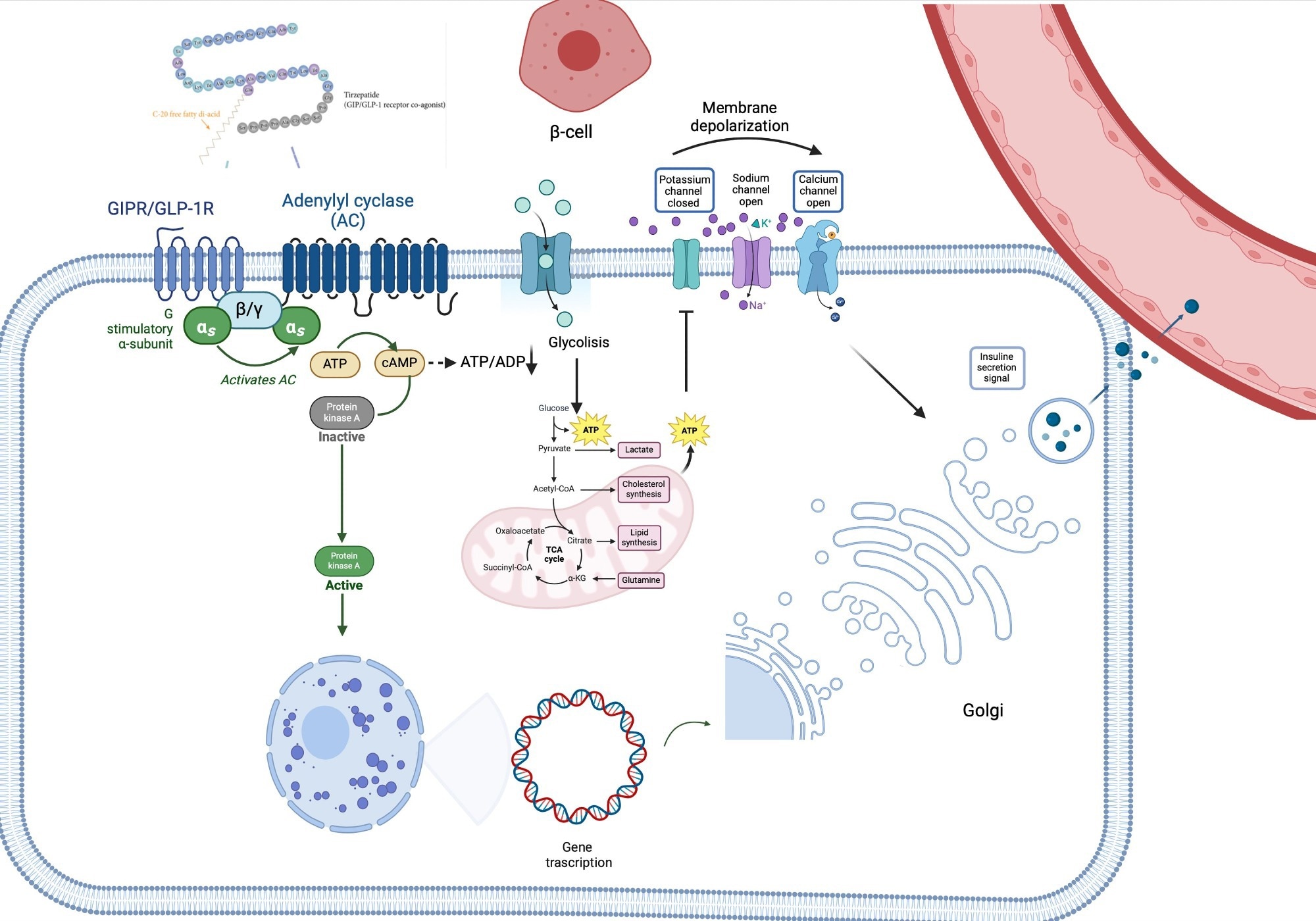
Tirzepatide’s pathway signaling. TZP binds its receptor, leading to the activation of adenylyl cyclase-cAMP-protein kinase A (PKA) pathway and thus stimulating glucose metabolism (glycolysis and Krebs Cycle). The increase of intracellular ATP levels hesitates in the closure of plasma membrane K+ channels, thus triggering β-cell depolarization. Due to depolarization, voltage-gated Ca2+ channels become open, favoring the entrance of Ca2+ into the cell, which concomitantly stimulates the releasing of calcium from the endoplasmic reticulum. This leads to the release of insulin into the bloodstream. Additionally, PKA stimulates insulin gene transcription, leading to insulin synthesis. αs, in vivo-subunit; ADP, adenosine diphosphate; ATP, adenosine triphosphate; β/γ, G protein β/gamma subunits; cAMP, cyclic adenosine monophosphate; GIP-R/GLP-1R, gastric inhibitory polypeptide receptor/glucagon-like peptide 1 receptor; PKA, adenylyl cyclase-cAMP-protein kinase A. Study: Tirzepatide against obesity and insulin-resistance: pathophysiological aspects and clinical evidence.
What is obesity, and why must we be concerned?
Obesity is an alarmingly common chronic weight gain disorder characterized by excessive fat deposition that often increases the risk of type 2 diabetes (T2D) and cardiovascular diseases (CVD). Clinically defined and diagnosed as having a body mass index (BMI) exceeding 30 kg/m2, the condition has rapidly risen in the global human population from 4% in 1975 to an astounding 18% (more than quadruple) in 2016. The World Health Organization (WHO) estimates that 59% of European adults (29% of males and 27% of females) are either overweight (BMI > 25 kg/m2) or obese.
Decades of research have highlighted the clinical demerits of abnormally high body weight (BW), with BMIs exceeding 30 kg/m2 and 40 kg/m2 correlated with decreased life expectancies of three and 10 years, respectively. BW higher than 22.5 kg/m2 has been observed to increase CVD and T2D risk substantially, contributing to more than 30% of global human mortality. High BW has further been implicated in impaired bone health, reproductive performance, and the genesis of certain cancers. Obesity pathophysiology is multifactorial and involves social, psychological, and behavioral factors, genetic and metabolic predisposition. Energy intake exceeding expenditure, along with factors such as miRNA dysregulation, plays a critical role. Together, these facts highlight the need for effective interventions to curb the spread of this silent epidemic.
How do we combat obesity?
Despite substantial research into the risk factors associated with overweight and obese outcomes, the multifactorial nature of these conditions hinders population-scale interventions against these conditions. Obesity has been observed to arise from a combination of social, genetic, metabolic, and psychological variables, with recent poor health behavior trends (diet and sedentary lifestyles) exacerbating the epidemic. Recently, research suggests the role of microRNAs (miRNAs) – small, non-coding RNA molecules involved with post-transcriptional gene expression – in altering the course of obesity pathophysiology. However, this recent is still nascent, and the mechanistic underpinnings remain poorly understood.
It is thus imperative that interventions aimed at treating, and not just preventing, obesity are developed. Barre J. L. Campo pioneered research in this field, discovering in the early 1930s that a class of peptides called ‘incretins’ could promote β- cells’ insulin release, promoting blood-sugar metabolism, appetite regulation, and subsequent weight loss. This discovery has proven critical in the development of pharmaceutical interventions against obesity.
What is Tirzepatide, and how is it a ‘silver bullet’ against obesity?
The glucose-dependent insulinotropic polypeptide (GIP) and the glucagon-like peptide-1 (GLP-1) are the best-studied and most commonly used incretins. Naturally released by the human gut and vital in appetite regulation and weight management, research has revealed that supplementation in obese patients can help reduce the latter’s BW by 20% or more. Hitherto, these incretins were used separately with their dosage depending on patients’ BW and drug response.
Tirzepatide (TZP; LY3298176) is a novel pharmacological innovation developed by Eli Lilly and Company in 2016 that combines both GLP-1 and GIP into a single subcutaneous weekly injection. Its chemical formula is C225H348N48O68, a synthetic peptide with 39 amino acids, allowing a single weekly subcutaneous administration due to its long half-life. The present review explores the in vitro and in vivo benefits of Tirzepatide’s effects, with notes on the drug’s pleiotropic effects on other organs. It focuses on the SURPASS and SURMOUNT clinical trial programs, presently the best evaluations of Tirzepatide’s clinical efficacy.
Tirzepatide’s pathophysiological effects
Thus far, in vitro preclinical trials have been conducted on rat β-cells, recombinant GLP-1R and GIP-R-expressing cell lines, and human islets. These studies have demonstrated that Tirzepatide’s combination of GLP and GIP promotes insulin sensitivity, appetite suppression, and cyclic adenosine monophosphate (cAMP) metabolism significantly better than administering either single agent (GLP or GIP). This results in substantially improved weight loss (WL) compared to conventional WL drugs.
In vivo studies on murine models confirm the above results and highlight the drug’s long-lasting weight-reduction effects. In obese mice, Tirzepatide interventions have been shown to enhance β-cell proliferation and function, reduce glucotoxicity, and extend life expectancy.
“Pleiotropic effects of GIP receptor stimulation in other tissues, mediated by mechanisms other than typical protein G-coupled receptor pathways, might bring additional benefits. Acting on insulin and glucagon levels, incretins, and thus TZP, may have indirect effects also on the liver and muscle. Experimental data on animal models have suggested that GIP suppresses peripheral arterial remodeling, thus showing an anti-atherosclerotic activity, by acting on receptors in the heart and vessels.”
Outcomes of clinical trials
The first clinical trial to test the clinical efficacy of TZP was the SURPASS program, a six-stage trial conducted on three separate cohorts – Japanese (SURPASS-J), Asian-Pacific (SURPASS-AP), and the cardiovascular outcome trial (SURPASS-CVOT). In these trials, the efficacy and safety of three decisive doses of TZP (5, 10, and 15 mg of TZP/week) were compared to conventional WL incretins, basal insulin, or placebos. In all the trials, TZP outperformed its comparators in HbA1c outcomes (reductions), diabetes reductions, WL, and risk of adverse cardiovascular events. For example, in the SURPASS-2 study, TZP at the dose of 5, 10, and 15 mg reduced HbA1c by -2.18% vs -1.86% with semaglutide and weight by -9.3 kg vs -5.7 kg.
The ongoing SURMOUNT trials confirm the results of the SURPASS trials. These trials represent studies specifically designed to assess the efficacy and safety of TZP in obesity management. Phase one of this four-phase trial has already concluded that TZP reduced systolic blood pressure (SBP) in 2,539 obese patients compared to placebos. Notably, TZP was additionally correlated with reductions in patients’ plasma lipid concentrations, waist circumferences, and fasting insulin levels.
Conclusions
TZP marks a revolution in WL and insulin treatments for overweight and obese patients, far surpassing the clinical efficacy of conventional interventions. Preclinical trials and clinical assessments of the drug have produced remarkable results, prompting the United States Food and Drug Administration (FDA) to approve its use as a first-in-class medicine in May 2022. Subsequently, the drug has been approved across the European Union (September 2022), Canada (November 2022), and Australia (December 2022). While the ongoing SURPASS clinical trial aims to elucidate the mechanistic underpinnings of the drug and the best dosages for treating patients of varying BMIs, its benefits cannot be understated.










{kind=link}